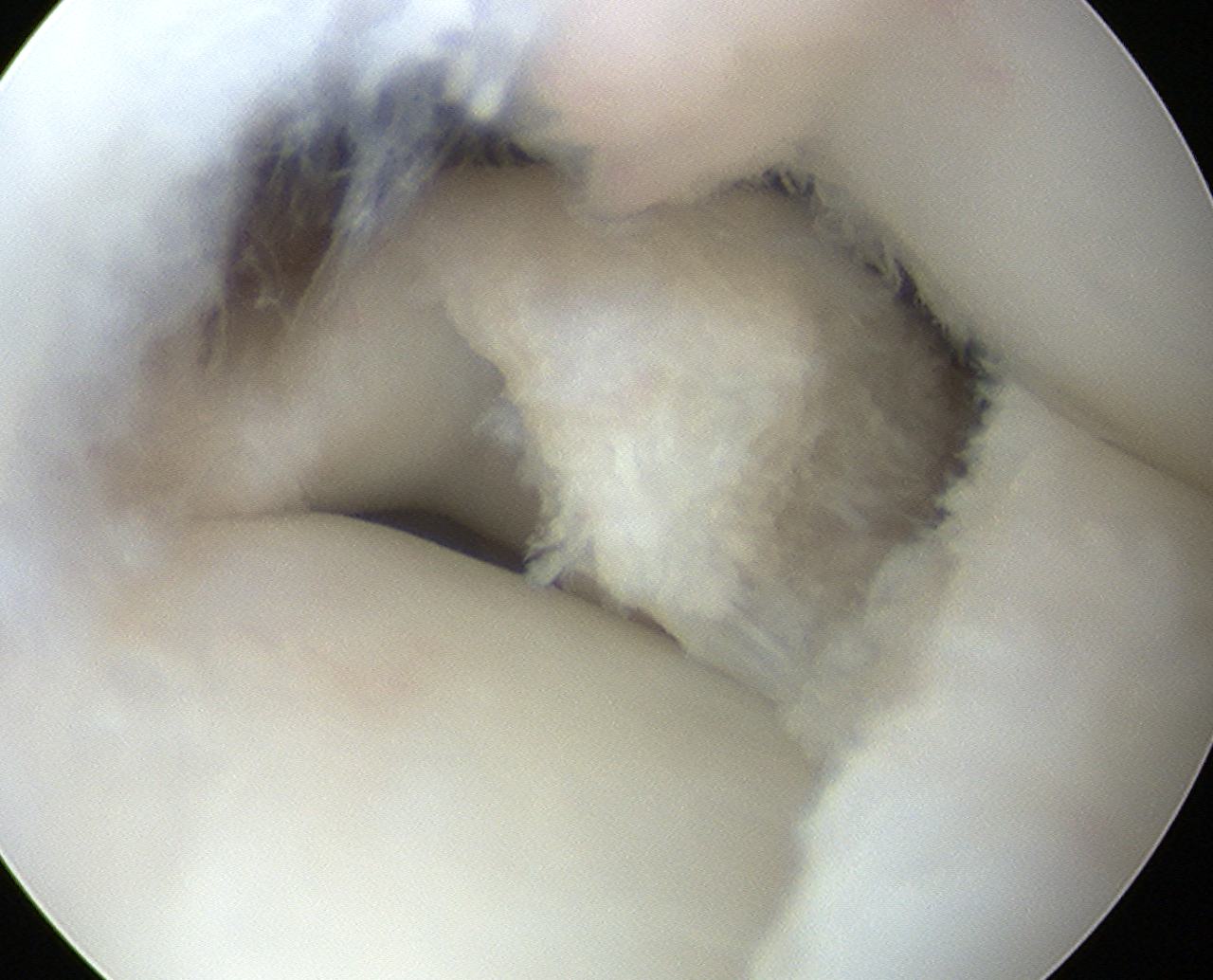
Definition
Round or "D" shaped rather than crescenteric meniscus
- occupies > 70% of tibial surface
- 90% occur on lateral side
Epidemiology
Uncommon
- 1:100
- usually presents in children & adolescents
Case reports of
- medial
- bilateral
- medial and lateral in same knee
Aetiology
Controversial
Theories
1. Failure of resorption of embryological meniscus centre
- however the lateral meniscus is never discoid during normal development
2. Lack of normal fixation to posterior tibia
- discoid shape 2° hypertrophy of posterior horn
- due to excessive motion
Presentation
1. Younger patients / adolescents < 15
- pain is commonest complaint
- clicking over lateral side
- recurrent effusions
- locking
2. Adults
- may never be symptomatic
- some adults present with MRI showing discoid meniscus
- theory that meniscus is protective in these people
- have gone most of life without tearing meniscus
- only resect if unstable tear
Signs
Reproduce clicking at 110° flexion
Lateral joint line tenderness / mass
Effusion
Limitation of extension / FFD
Classification Watanabe
1. Complete
- entire articular surface of tibial plateau covered by thickened abnormal meniscus
- minimal symptoms
- stable - i.e. capsular attachments intact
2. Incomplete
Normal peripheral attachments but not as extensive as complete type
3. Wrisberg Type
Unstable
- large posterior horn with no attachment to tibial plateau
- entire posterior portion hyper-mobile
- only attachment is Wrisberg Ligament
Most symptomatic
- displaced into intercondylar notch in extension
X-ray
Widened joint space

Flattening or cupping of plateau
Flat LFC
Hypoplastic Lateral Tibial Spine
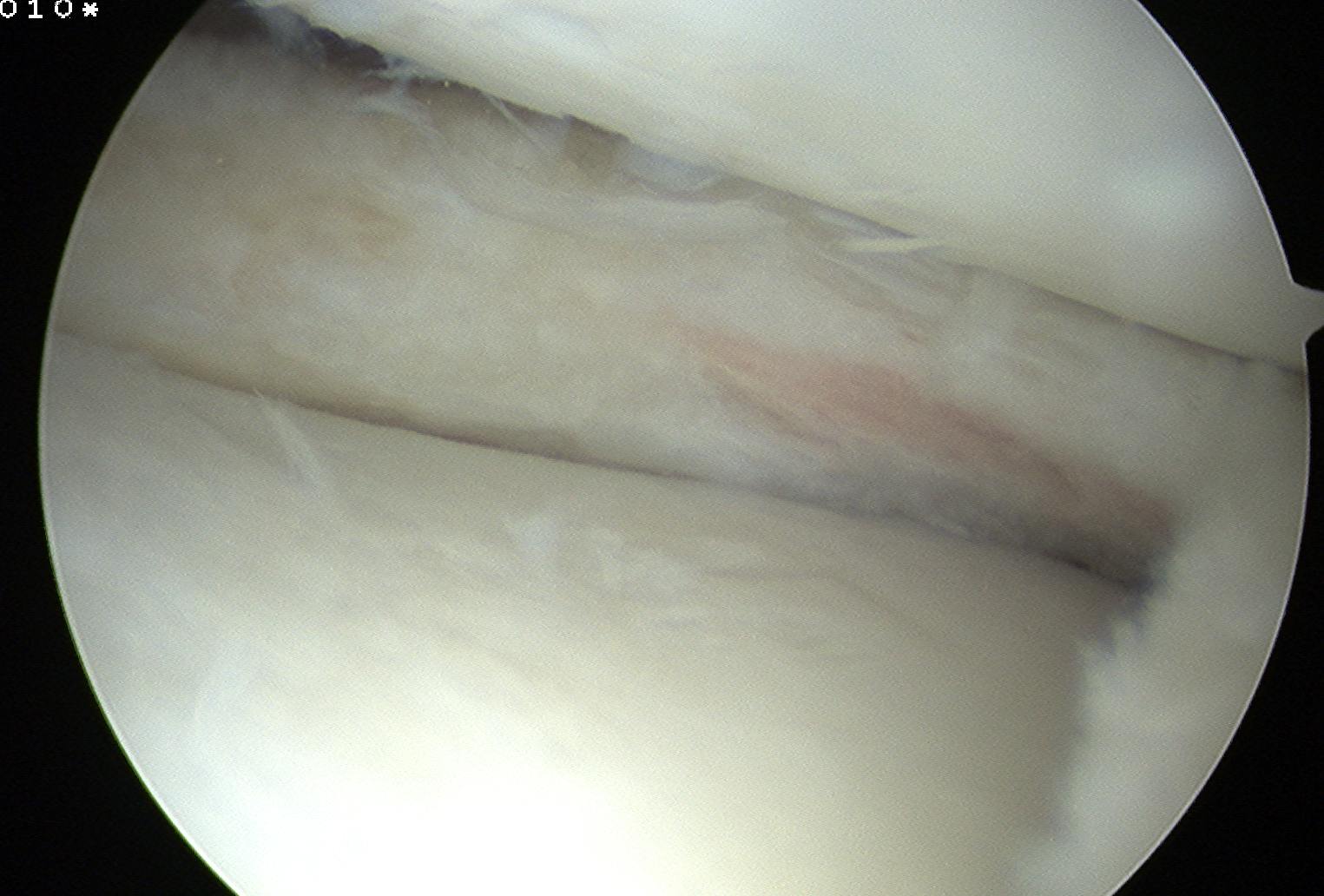
MRI
Obviously enlarged LM
See meniscus on 3 consecutive cuts




Management
Issue
There is a protective element to lateral meniscus
- resect only if painful tear / young patient
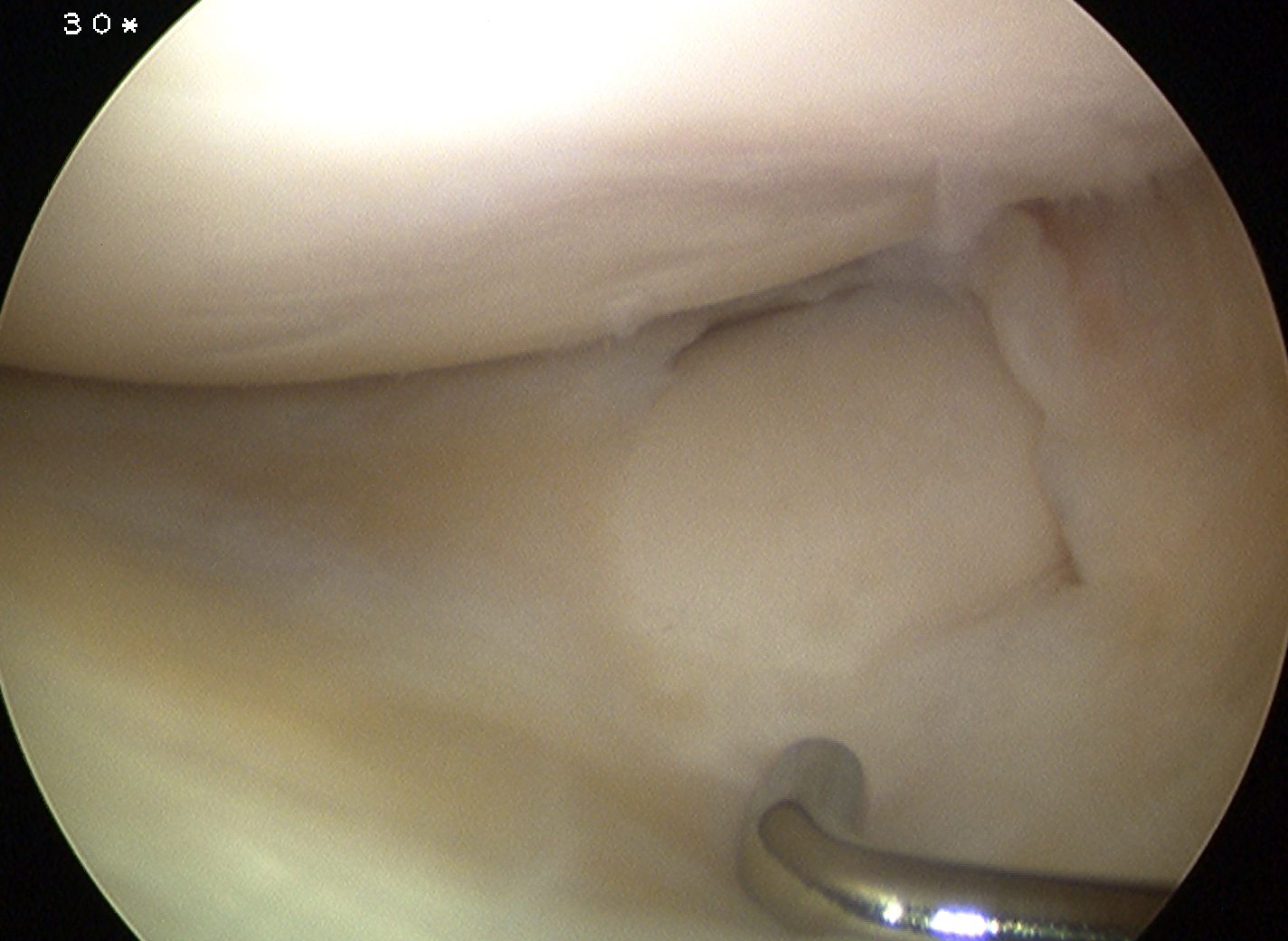
Aim
Convert unstable meniscus to a stable contoured one
Options
1. Stable
- partial central meniscectomy / saucerisation
2. Unstable (Wrisberg type)
- posterior capsular stabilisation / repair +/- saucerisation
Ahn et al Arthroscopy 2008
- 23 patients treated with posterior repair and partial central meniscectomy
- no reoperation at 51 months
- good symptomatic relief
3. Prophylactic meniscectomy
- no role
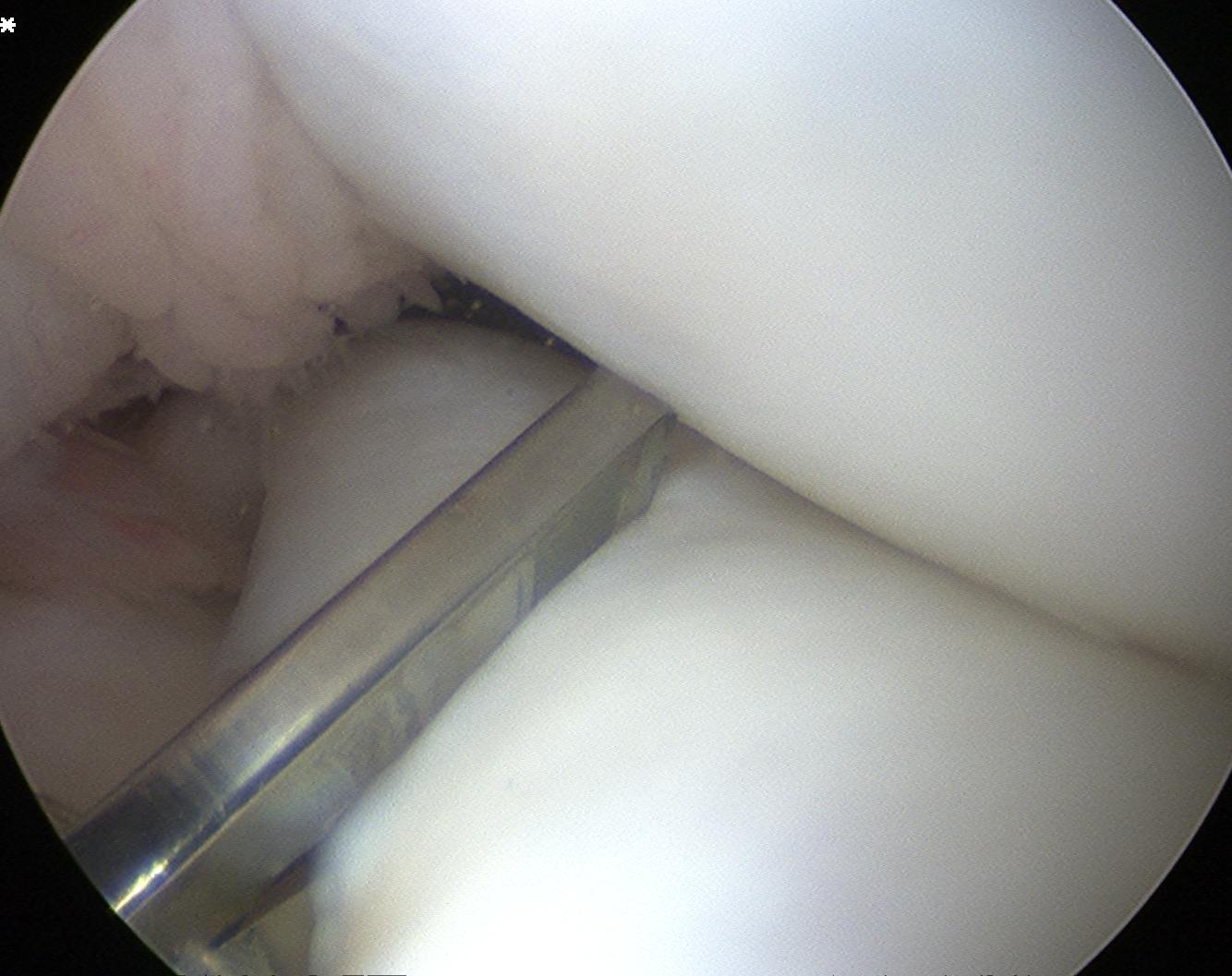
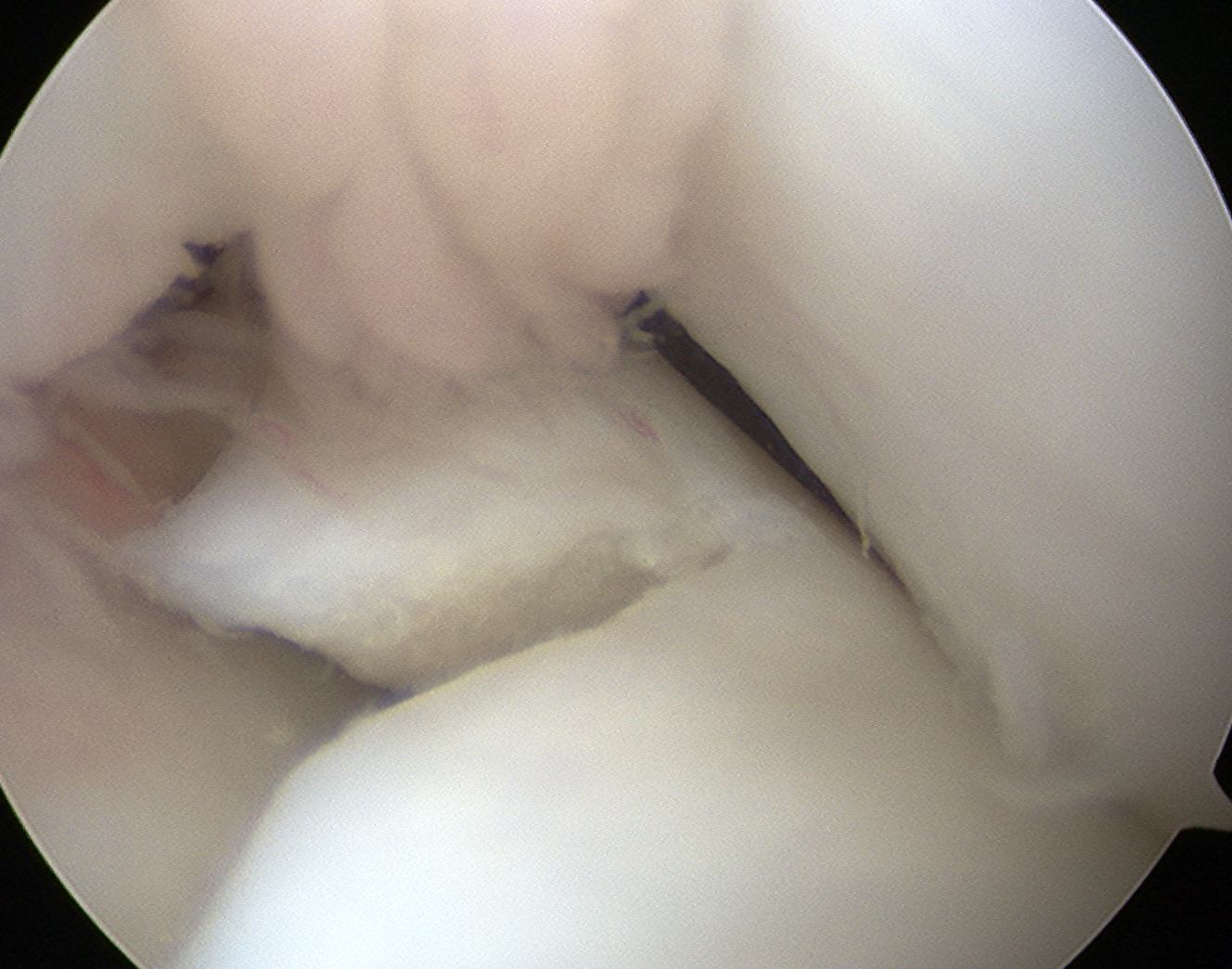
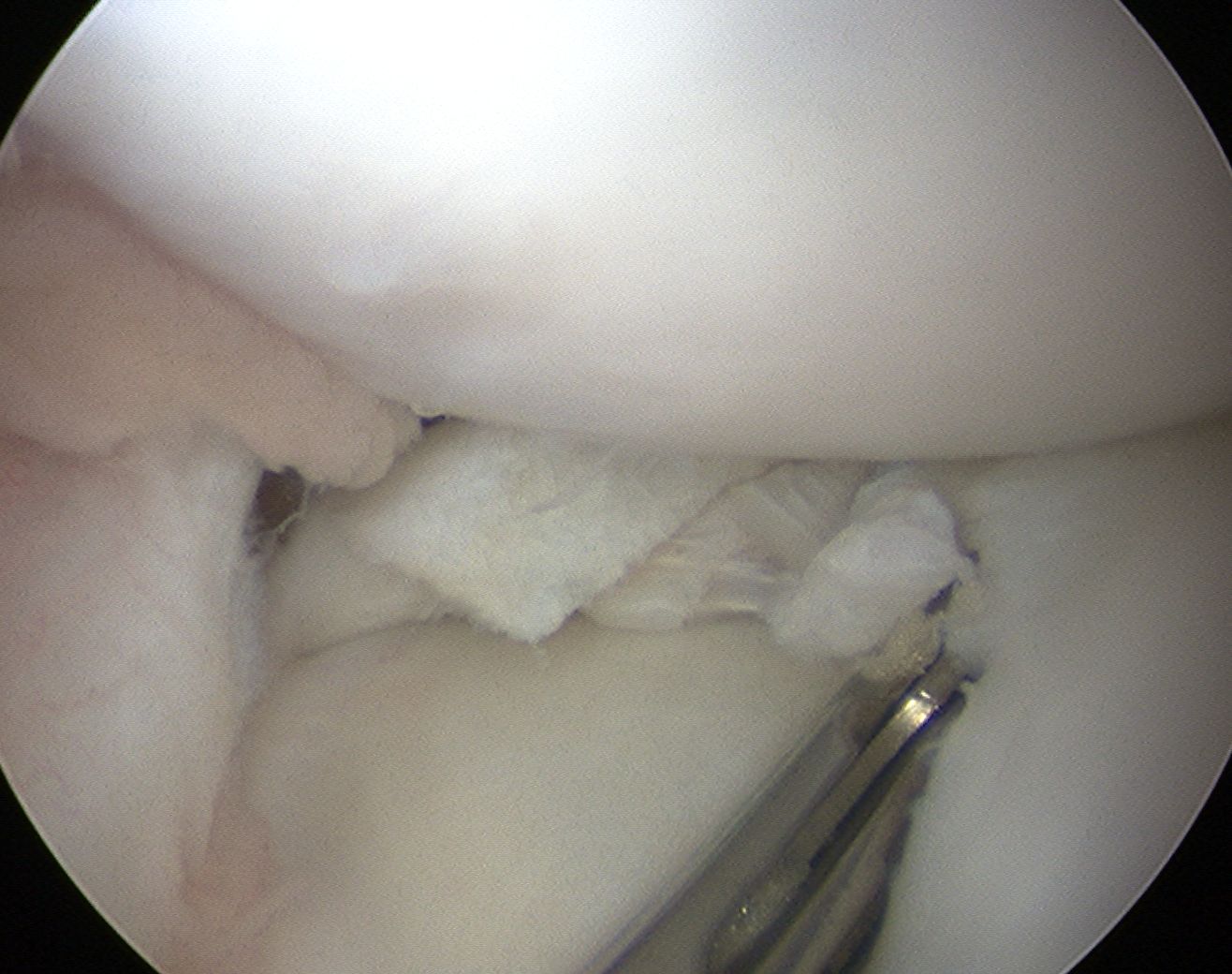
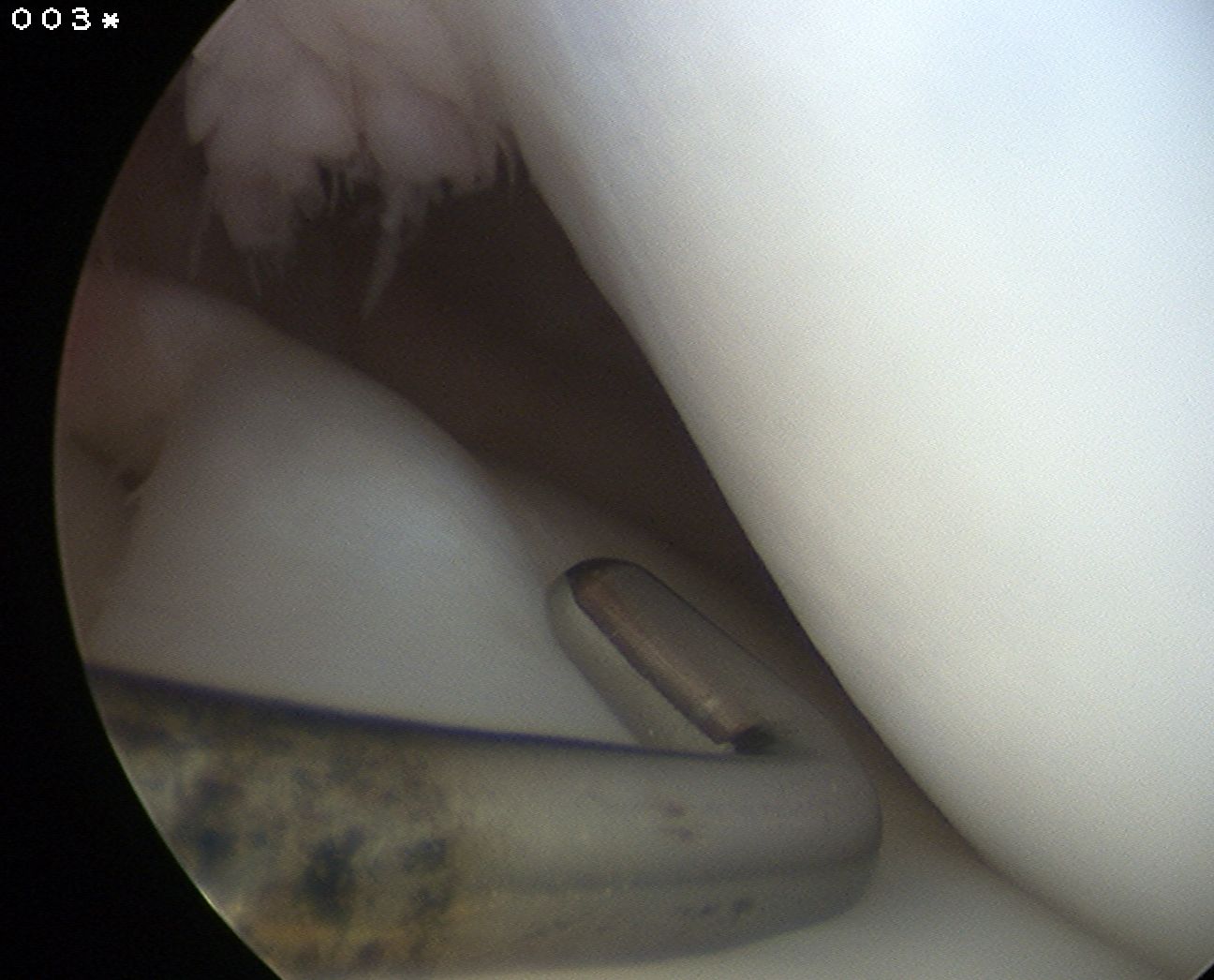
Technique Saucerisation
Issues
- demanding and technically difficult
- takes 1 - 2 hours
- difficult to know how much to resect
- need to ensure don't damage chondral surfaces
- reported cases of rapid and severe chondrolysis post resection in young patients
Technique
- make incision with scissors in medial aspect
- resect posterior part
- saucerise laterally and anteriorly
- need to ensure don't detach anterior horn