
Definition
Developmental dysplasia of the hip
- the femoral head does not have the normal relationship with the acetabulum
- the acetabulum is dependent on the femoral head for normal development
Four clinical patterns
| Hip instability | Acetabular dysplasia | Subluxed hip | Dislocated hip |
|---|---|---|---|
| Looseness / laxity |
Normal relationship of the hip Acetabulum shallower and more vertical |
Non concentric contact between femoral head and acetabulum
Reducible or irreducible |
No contact between femoral head and acetabulum
Reducible or irreducible |
Epidemiology
Hip instability 1%
- 5/1000 males
- 13/1000 females
- 90% resolve spontaneously
Unilateral 63% / left side 64%
75% of patients with DDH are female
Etiology
Tirta et al JAMA Netw Open 2025
- meta-analysis for risk factors of 64,000 DDH
- breech delivery / family history DDH / oligohydraminos / female
| Ligamentous laxity | Mechanical theory | Familial | Associated disorders |
|---|---|---|---|
|
Females
Progresterone rich environment
Familial hyperlaxity / collagen disorders
|
Breech / Twins
First born
High birth weight
Oligohydraminos
Swaddling |
12x increased risk with sister / daughter |
Larsen's / Arthrogryposis
Torticollis
Meta-tarsus adductus
Congenital knee dislocation |
Pathology
| Acetabular dysplasia | Femoral head | Capsule | Soft tissue |
|---|---|---|---|
|
Becomes vertical and shallow
Neolimbus - crest of new fibrocartilage - between true and false acetabulum |
Dislocates superior and posterior
Head deformed
Neck short and anteverted |
Capsule enlarged / stretched
Zona orbicularis - capsule narrows where iliopsoas crosses
|
Labrum thickened +/- inverted (limbus)
Ligamentum teres thicker
Pulvinar thickened
Transverse ligament pulled superior and forms blockage |
Natural history
Acetabular dysplasia - associated with early development of osteoarthritis (OA)
Hip subluxation - leads to OA in 30's and 40's
Hip dislocation
- articulates with ilium: very early OA
- no articulation with ilium: pain free but abnormal gait (bilateral waddling gait, unilateral short leg gait) until 40s
Screening
Clinical examination of the hips in all newborns
Any abnormal findings or high risk - ultrasound
Selective ultrasound screening
Indications
- positive clinical findings
- breech/ oligohydraminos / multiple births / family history DDH
- foot deformities (CTEV / metatarsus adductus), torticollis
Universal ultrasound screening
Issue - 90% unstable hips will resolve without treatment
- systematic review of universal v selective screening
- overall incidence late presenting DDH is 1/10,000
- universal screening reduced late presenting DDH
- universal screening increased incidence abduction bracing without reducing incidence later surgery
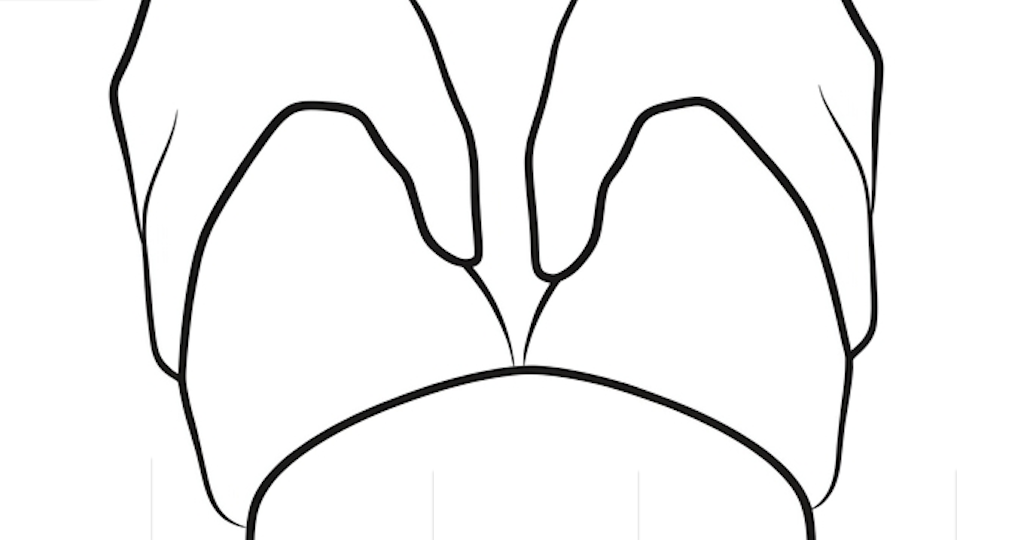
Examination neonate
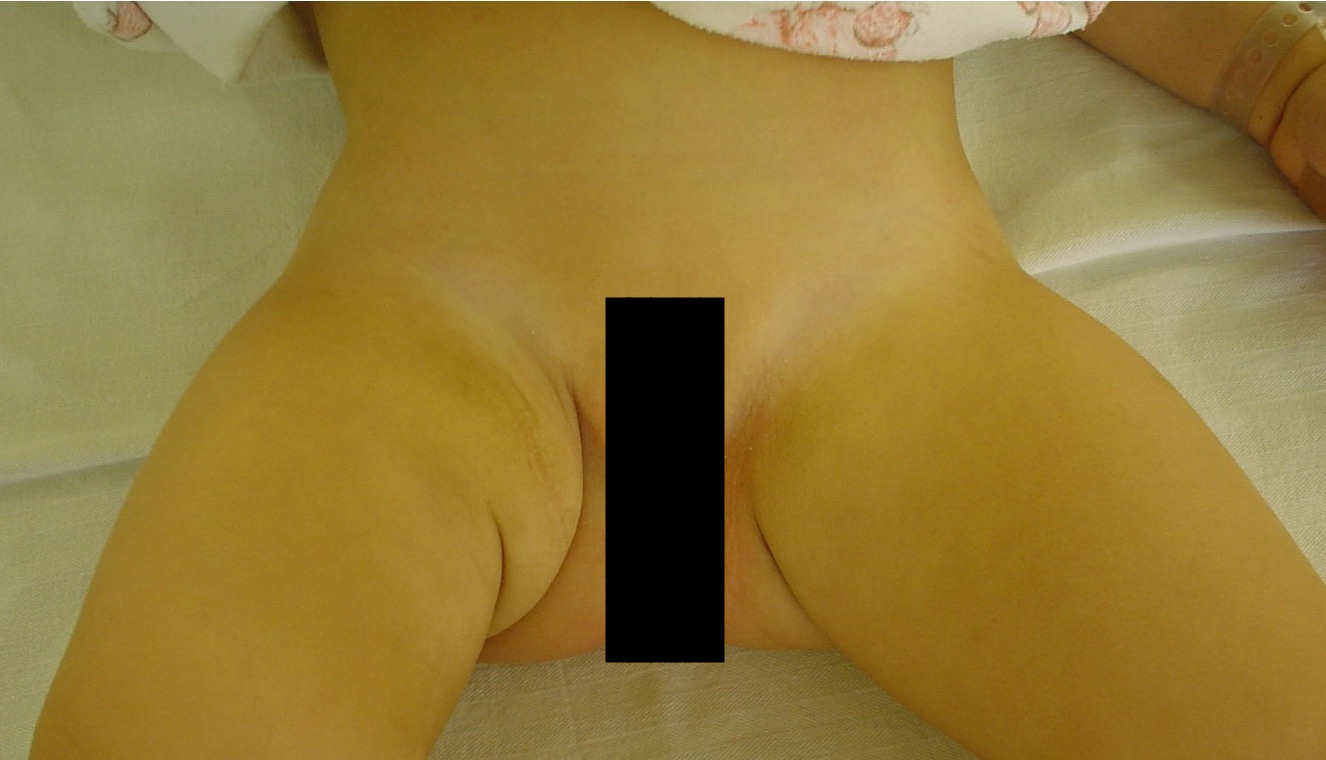
Asymmetric thigh folds / creases
Reduced abduction - normal abduction is 80 - 90°
Dynamic maneuvers
Hip is stable / subluxable / dislocated and reducible / dislocated and non-reducible
| Ortolani test | Barlow provocation test |
|---|---|
| Hip is Out, Ortolani test reduces hip | Push hip Back out with adduction and posterior force |
|
Thumb on adductor tubercle & ring finger on GT - hip and knee 90° flexion - abduct hip & lift GT forward - clunk of reduction felt |
One hand holds pelvis - adduction to 10o while axial pushing thigh backward - dislocates in this position over posterior acetabulum - feel clunk of dislocation - may feel sliding of subluxing hip |
Ortolani test: the hip is dislocated with the leg adducted
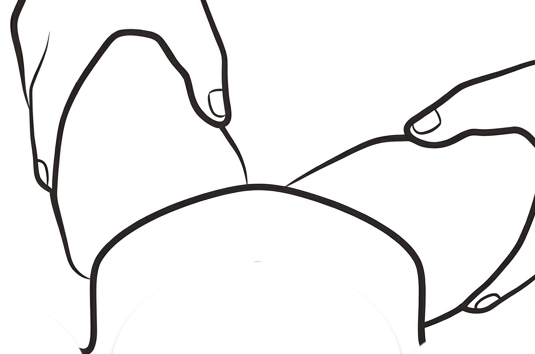
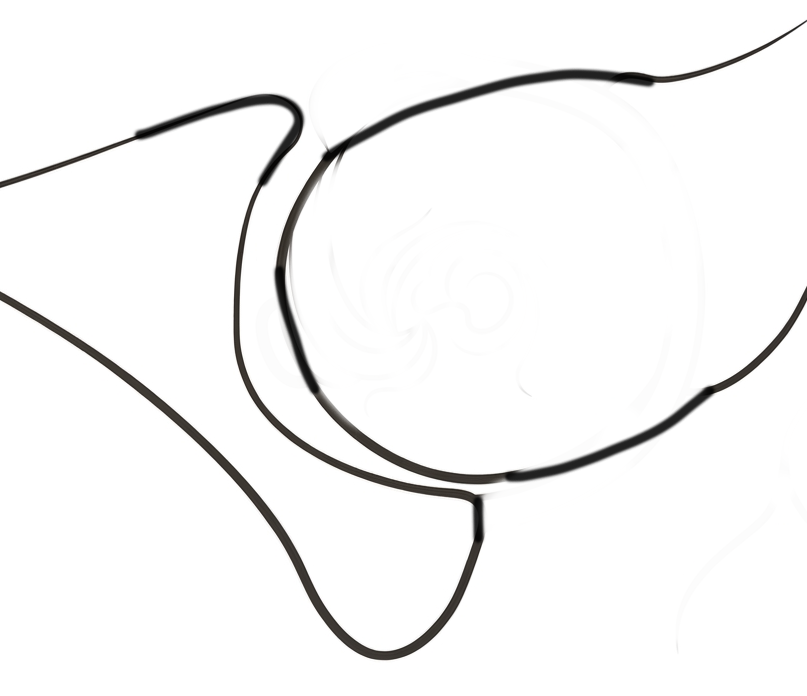
Ortolani test: feel the hip reduce with abduction
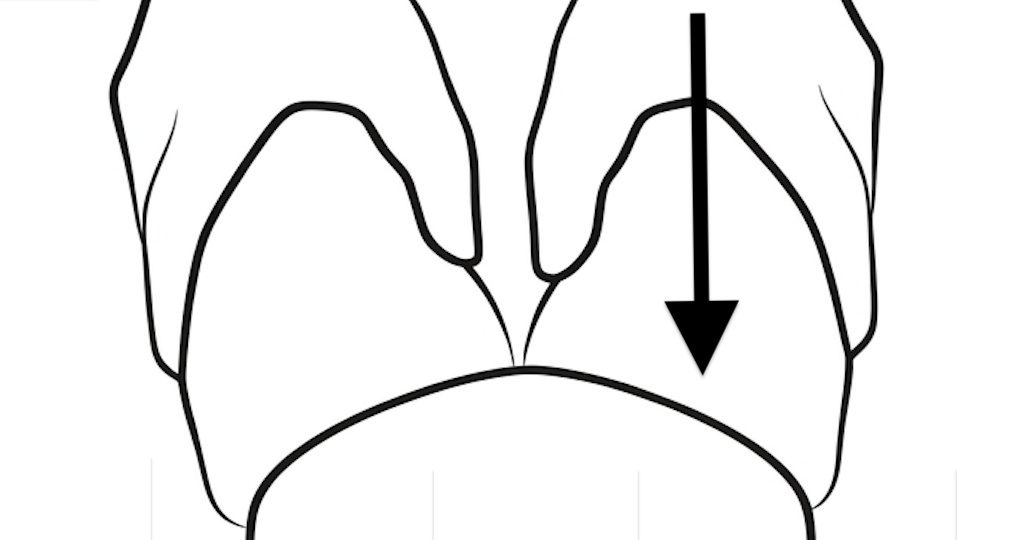
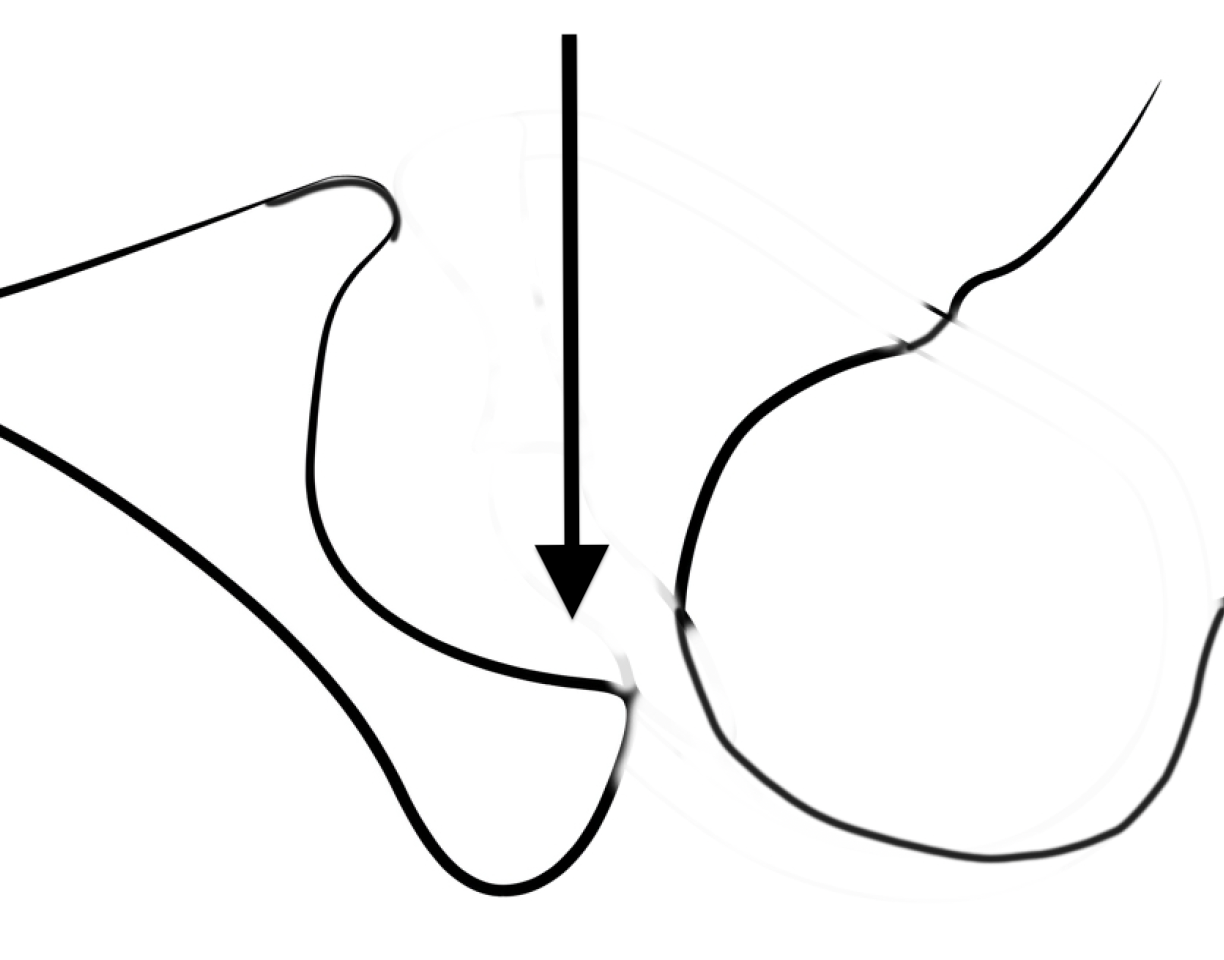
Barlow test: feel the hip sublux or dislocated with the hip adducted and a posterior force
Chavoshi et al Arch Bone Jt Surg 2022
- systematic review of examination findings in neonatal DDH
- sensitivity 37%, specificity 98%
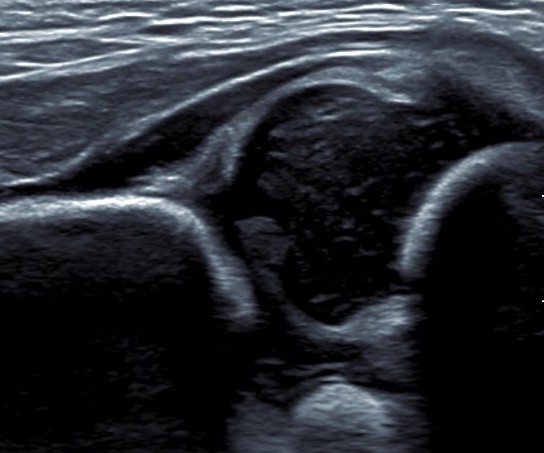
Ultrasound
Background
Best imaging before 4 - 6 months when superior femoral epiphysis cartilaginous
Chavoshi et al Arch Bone Jt Surg
- systematic review of accuracy of ultrasound in DDH
- sensitivity 93%, specificity 97%
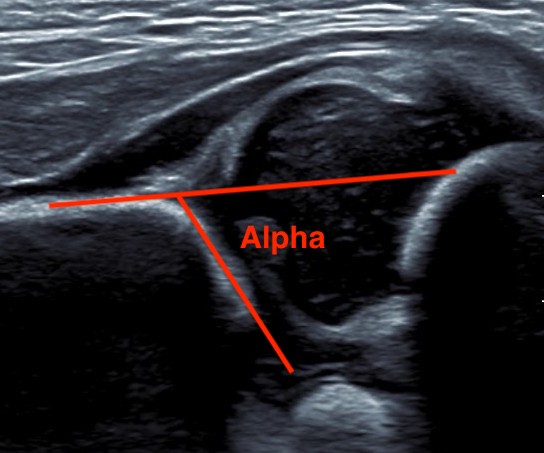
| Alpha Angle | Beta Angle | Dynamic |
|---|---|---|
|
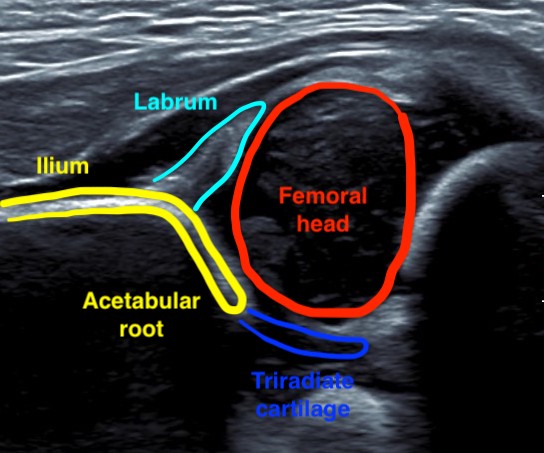
Between ilium & bony roof acetabulum
|
Between ilium & cartilage roof / labrum
|
Ultrasound Ortolani / Barlow
|
|
Normal > 60°
The lower the alpha angle, the more subluxed the hip is
|
Normal < 60o |
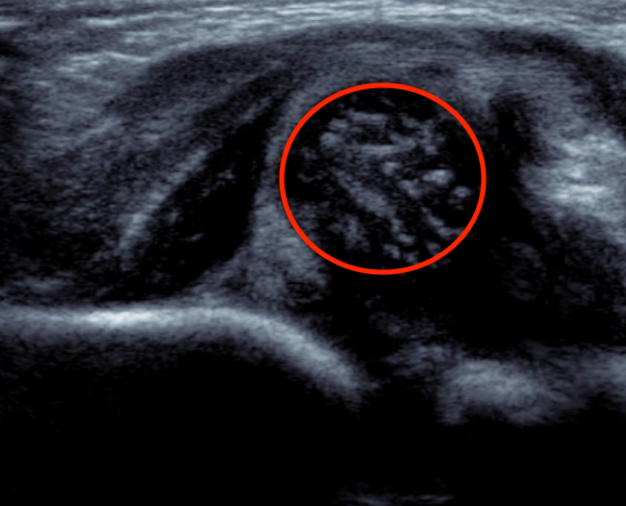
Alpha angle between ilium and bony roof of acetabulum
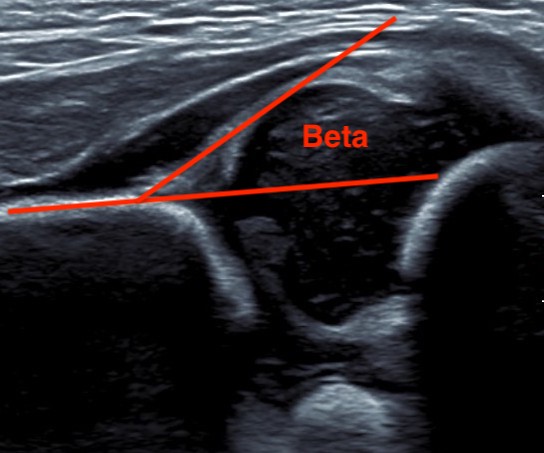
Beta angle between ilium and cartilage roof / labrum
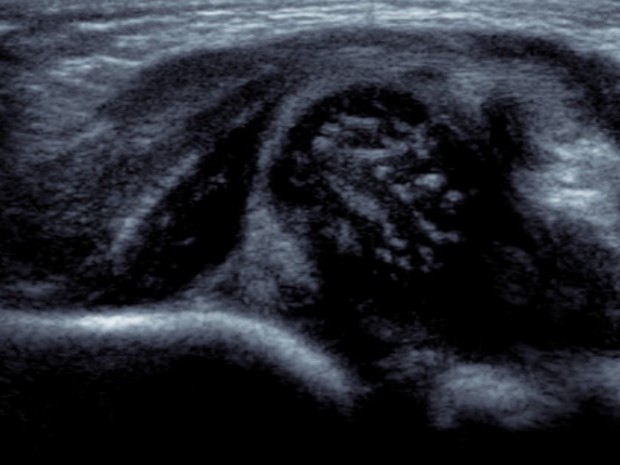
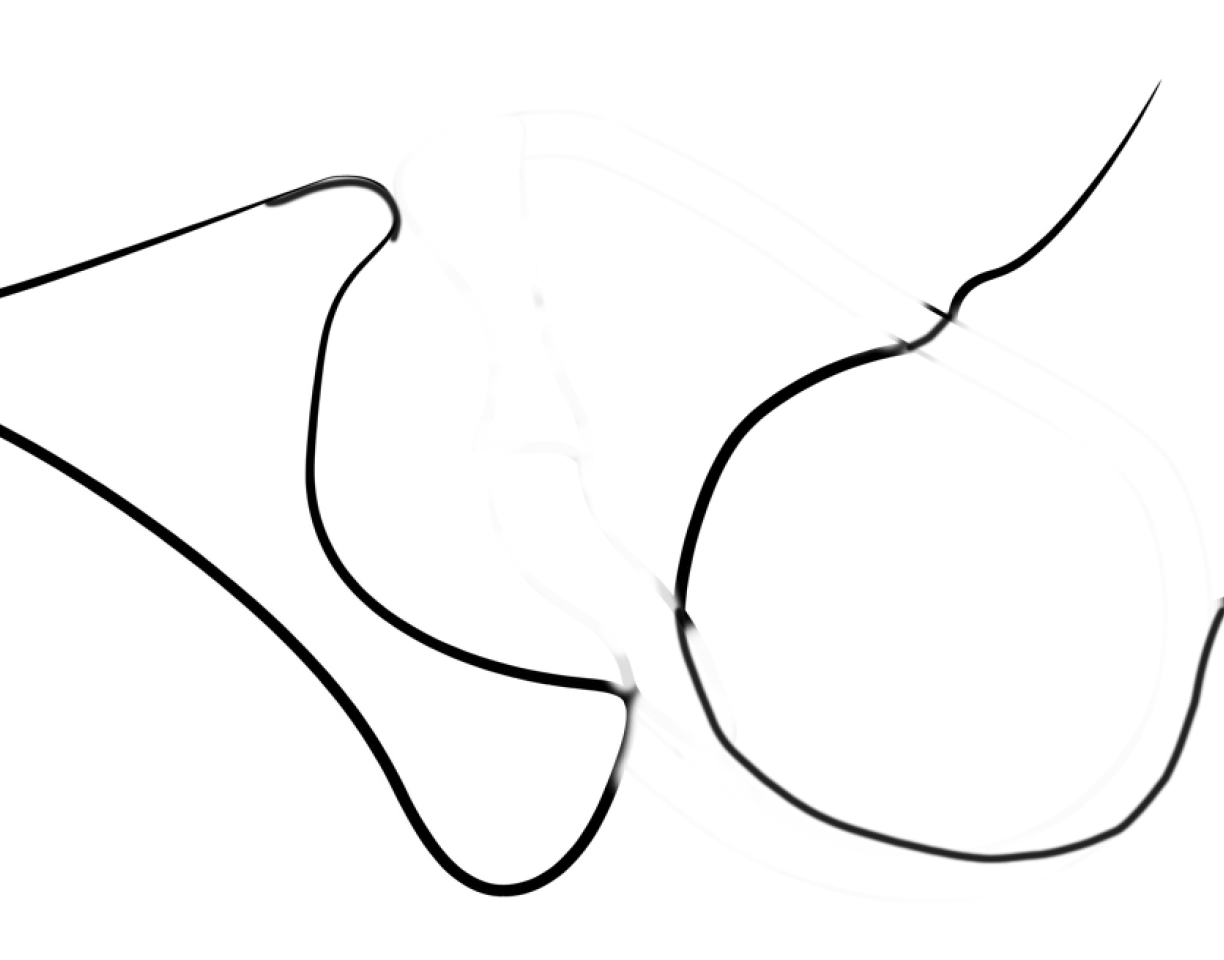
Dislocated hip on ultrasound
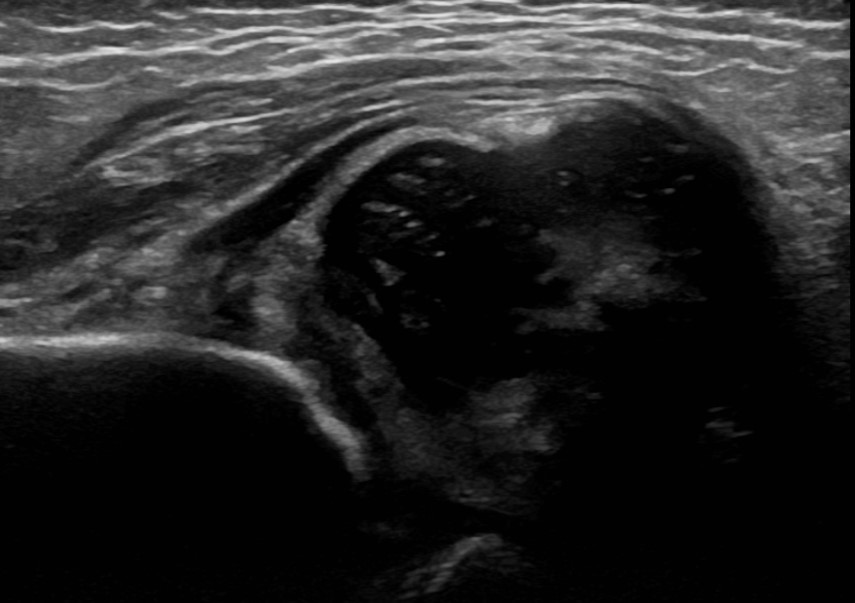

Dislocated hip on ultrasound
Graf Classification
| Alpha angle | Beta angle | Findings | |
|---|---|---|---|
| Type I | > 60 | < 55 | Normal |
| Type II | 43 - 60 | 55 - 77 | Delayed ossification SFE |
| Type III | < 43 | > 77 | Subluxed |
| Type IV | Unmeasurable | Unmeasurable | Dislocated |
AP X-ray
Timing
AP after 6 months of age when the superior femoral epiphysis becomes ossified
Create 4 quadrants on xray
- Hilgenreiner's Line - horizontal through triradiate cartilages
- Perkin's Line - vertical through lateral edge of bony acetabulum
- superior femoral epiphysis (SFE) should be in inner and lower quadrant
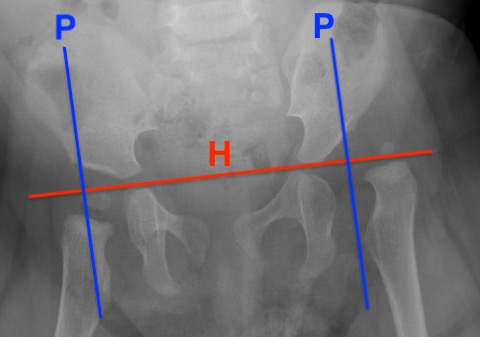
Dislocated hip with smaller superior femoral epiphysis (SFE) and location in the upper outer quadrant
Findings
| Superior femoral epiphysis | Disrupted Shenton's line | Increased acetabular index | Increased head to teardrop distance |
|---|---|---|---|
|
Smaller
In upper/ outer quadrant |
Line along inferior neck
Line inferior border superior ramus |
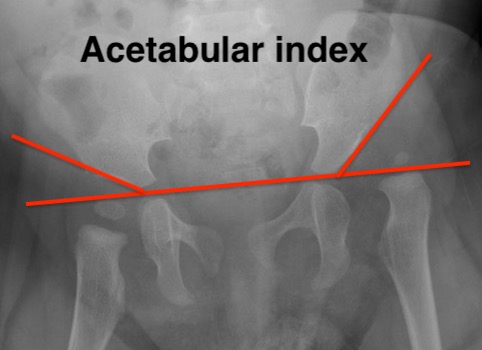
Angle between Hilgenreiner's line and acetabular line |
Lateral tear drop to medial ossification center |
|
Normal < 30° DDH > 35° |

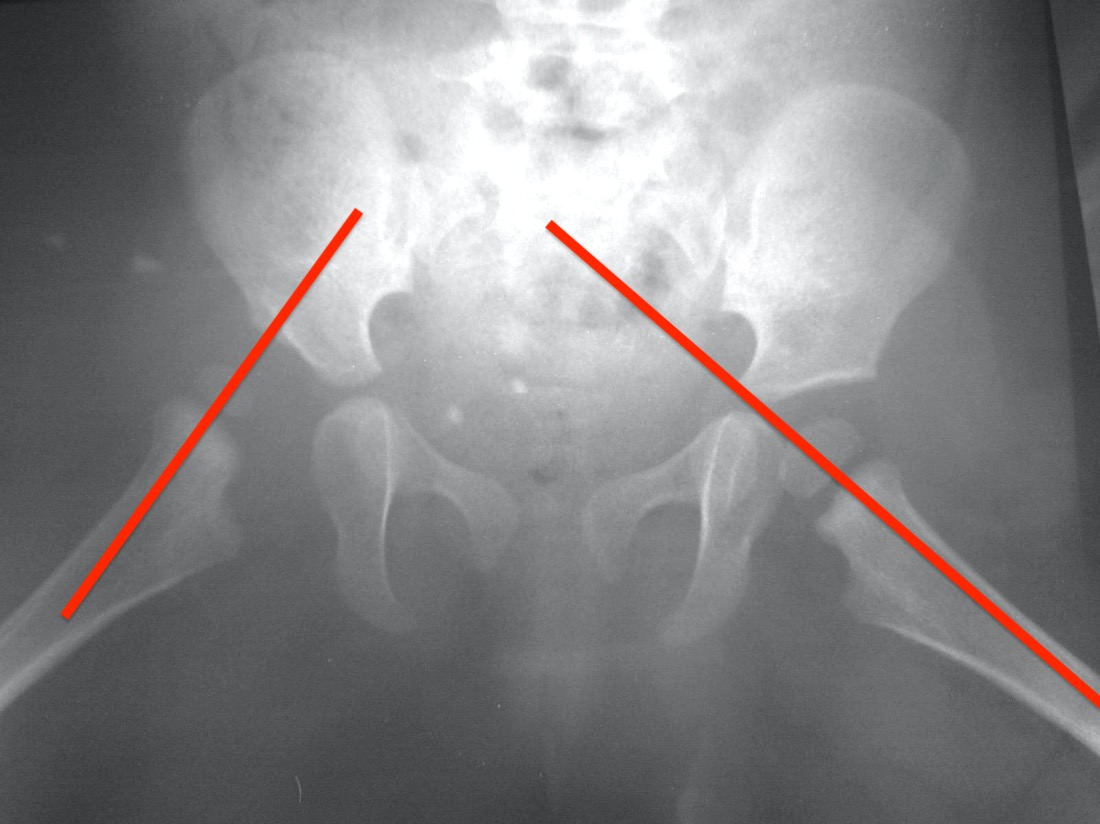
Von Rosen's view
Technique
AP pelvis with legs abducted 45° & IR 20°
Lines along femoral shafts should pass through center acetabulum & intersect at sacrum

Management
Principles
1. The older the age of treatment, the worse the outcomes
2. Acetabular potential for correction diminishes significantly after the age of 3 - 4
3. Aim to achieve a stable concentric reduction of the femoral head into the acetabulum without AVN
4. To correct acetabular dysplasia
Guidelines
0- 6 months: Splint
6 - 18 months: Closed +/- open reduction
18 months - 8: Open reduction + acetabular osteotomy +/- femoral osteotomy
Avascular necrosis

AVN of the femoral head on the right
Etiology
Always iatrogenic / the result of treatment
- doesn't occur in untreated DDH
- excessive abduction in splint or spica
- forceful closed reduction
- vascular damage during medial approach
- failure to adequately detension hip during open reduction (releases, femoral shortening osteotomy
Kalamachi and McEwan X-ray classification


| Type 1 | Type 2 | Type 3 | Type 4 |
|---|---|---|---|
|
Nucleus only Irregular fragmentation |
Lateral physis | Central physis | Whole physis |
| Head will be normal |
Early lateral fusion Femoral head neck short Valgus |
Femoral neck short / coxa breva Greater trochanter overgrowth Coxa vara |
Coxa breva Coxa vara |
Clinical outcome
Coxa breva / Coxa valga / Coxa vara
LLD
Trendelenberg gait