shoulder
Background
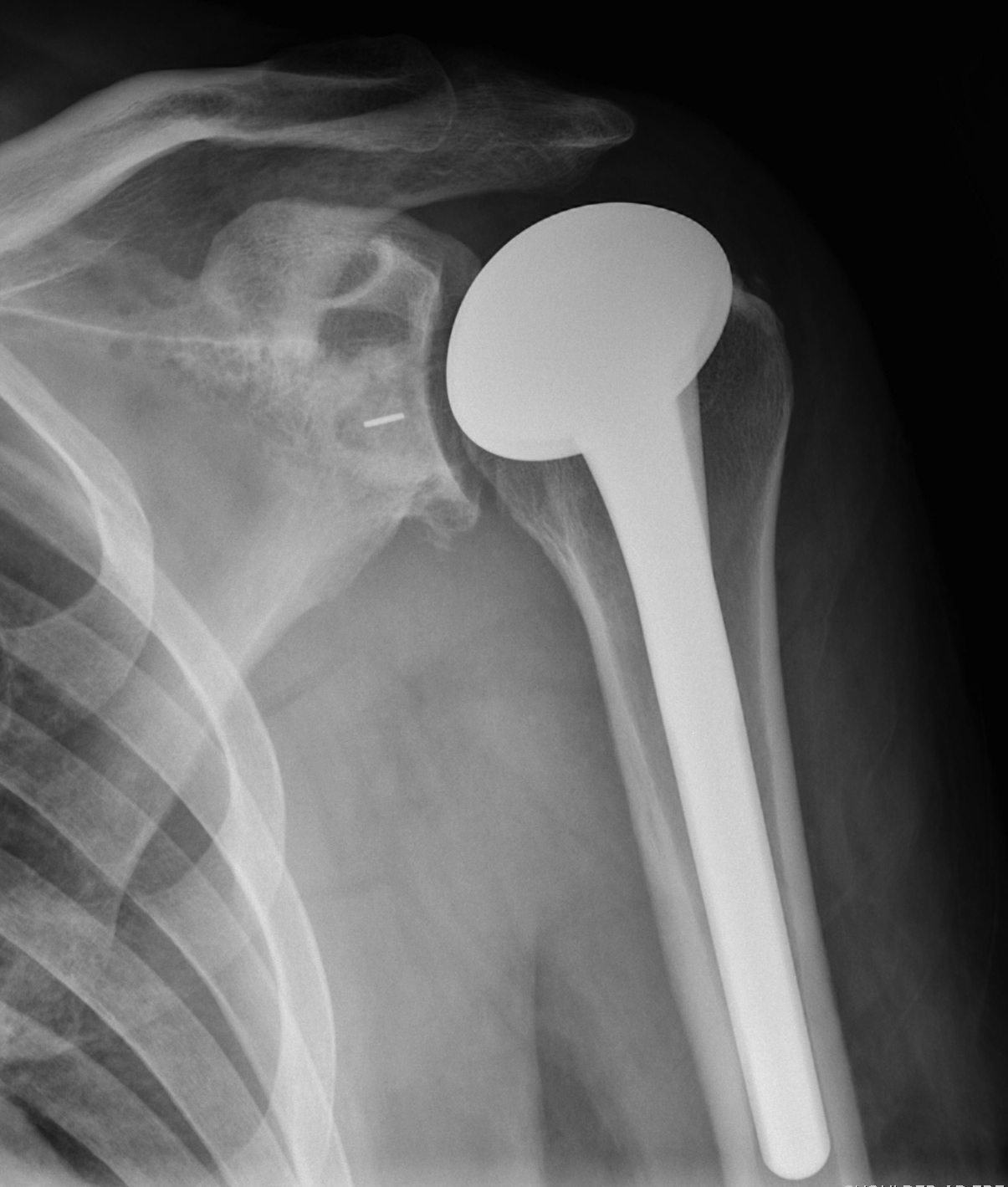

Indications
Osteoarthritis
Rheumatoid arthritis
Avascular necrosis
Remplissage
Indications
Engaging Hill Sachs
Shoulder
Approaches
Anterior
Anterolateral
Posterior
Anterior Approach / Deltopectoral
Indications
- shoulder stabilization
- arthroplasty
- fracture fixation
Approach
Position
- beach chair
- upper body elevated 30- 40o / reduces venous pressure and bleeding
Throwing Athlete
Throwing
Wind-up
- cocking
- ER up to 180o in pitcher
Acceleration
- large scapular muscles
- acceleration - 7000o/sec
- rotatory acceleration similar to car tyre at 130 kph
Control and deceleration
- fragile cuff & glenohumeral ligament complex
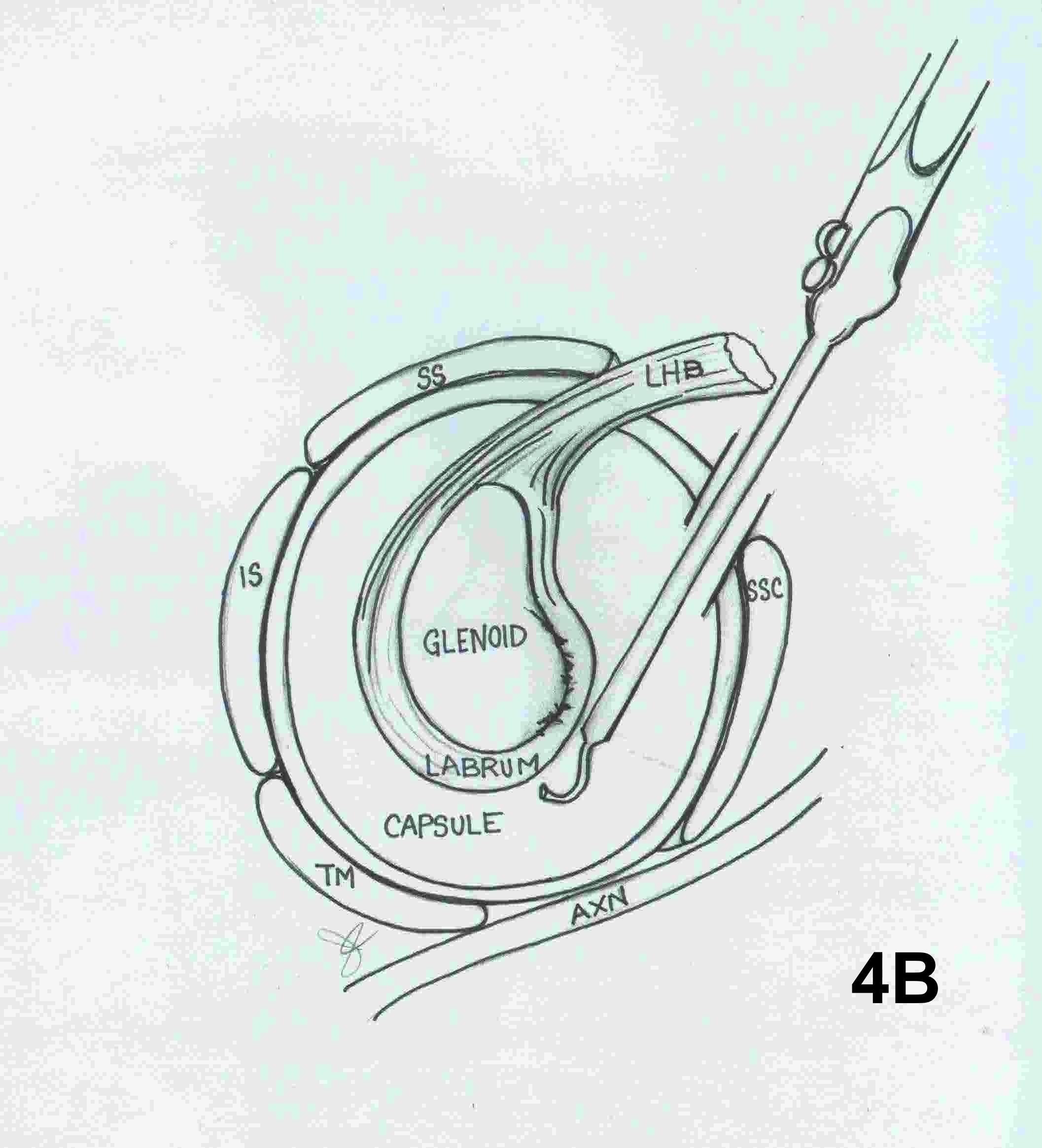
Anatomy
Synovial Osteochondromatosis
Definition
Chondroid Metaplasia of synovium affecting large joints
Nodules of hyaline cartilage
- formed in the subsynovial layer of joint capsules
Epidemiology
Rare lesion
Most common in 20's and 30's
Sex: M > F (2:1)
Monoarticular
Site
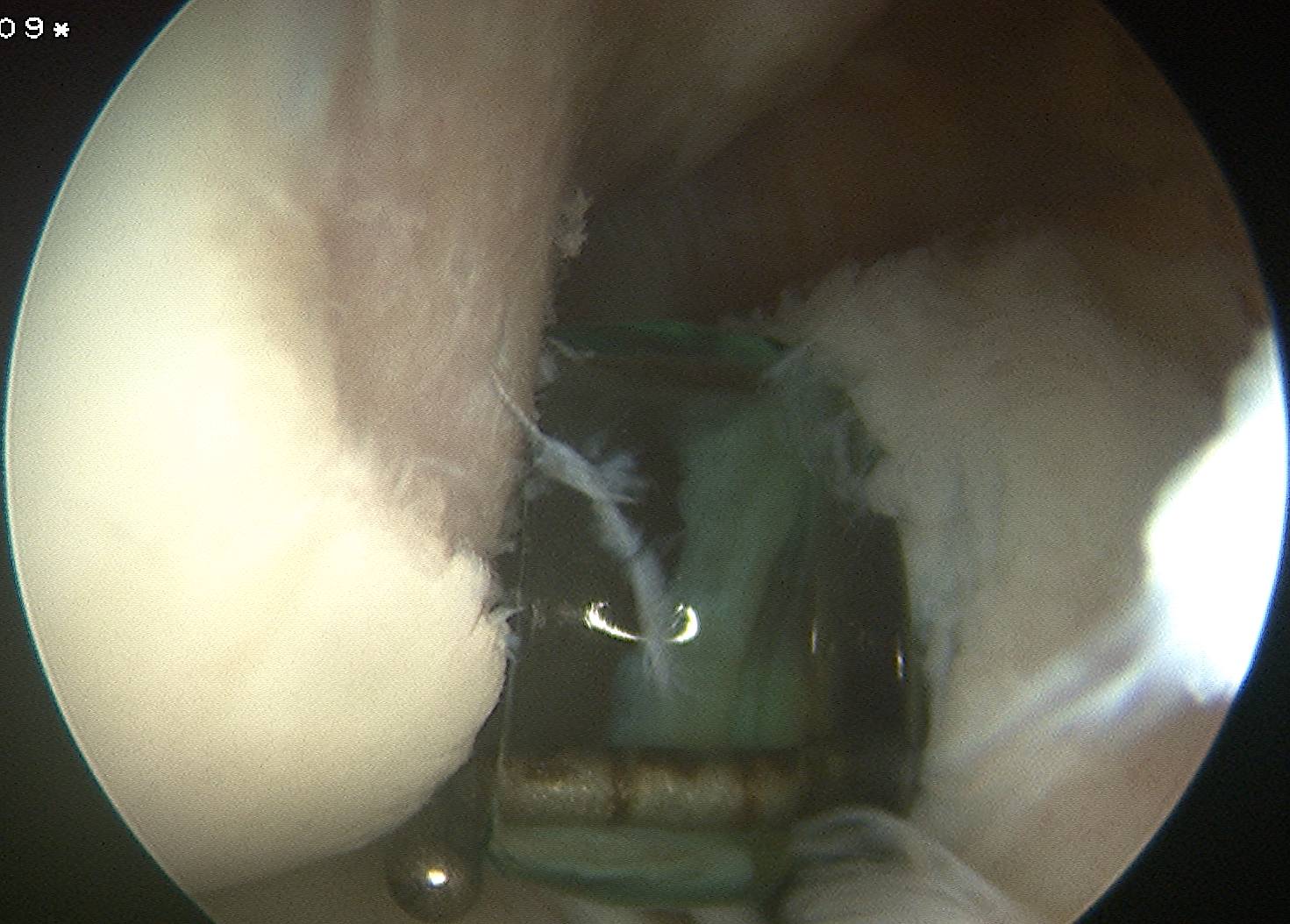
Arthroscopic Stabilisation

1. EUA
Compare both shoulders
- ROM
- anterior and posterior draw
- load and shift
- sulcus sign
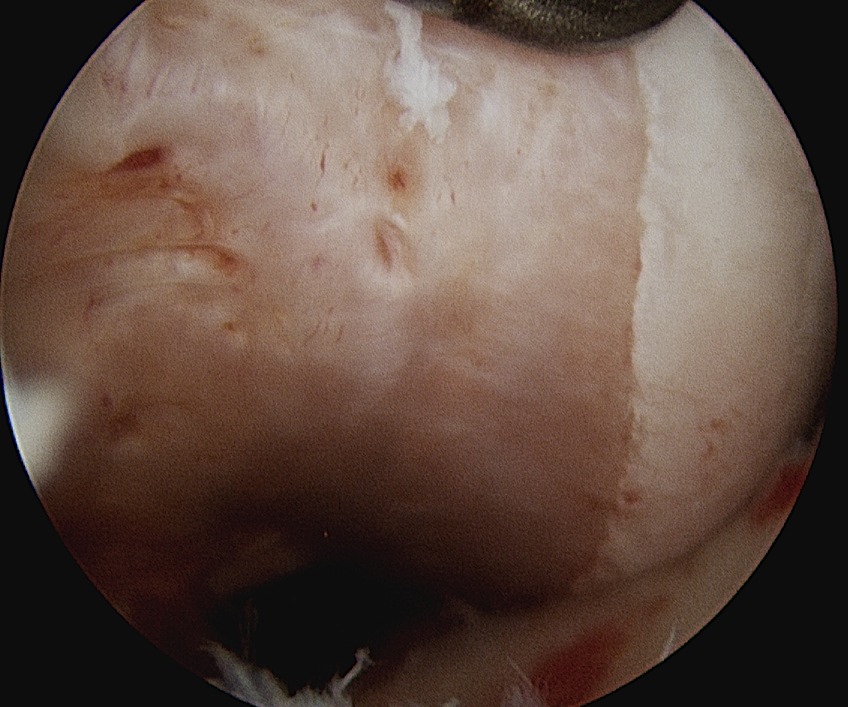
HAGL
Definition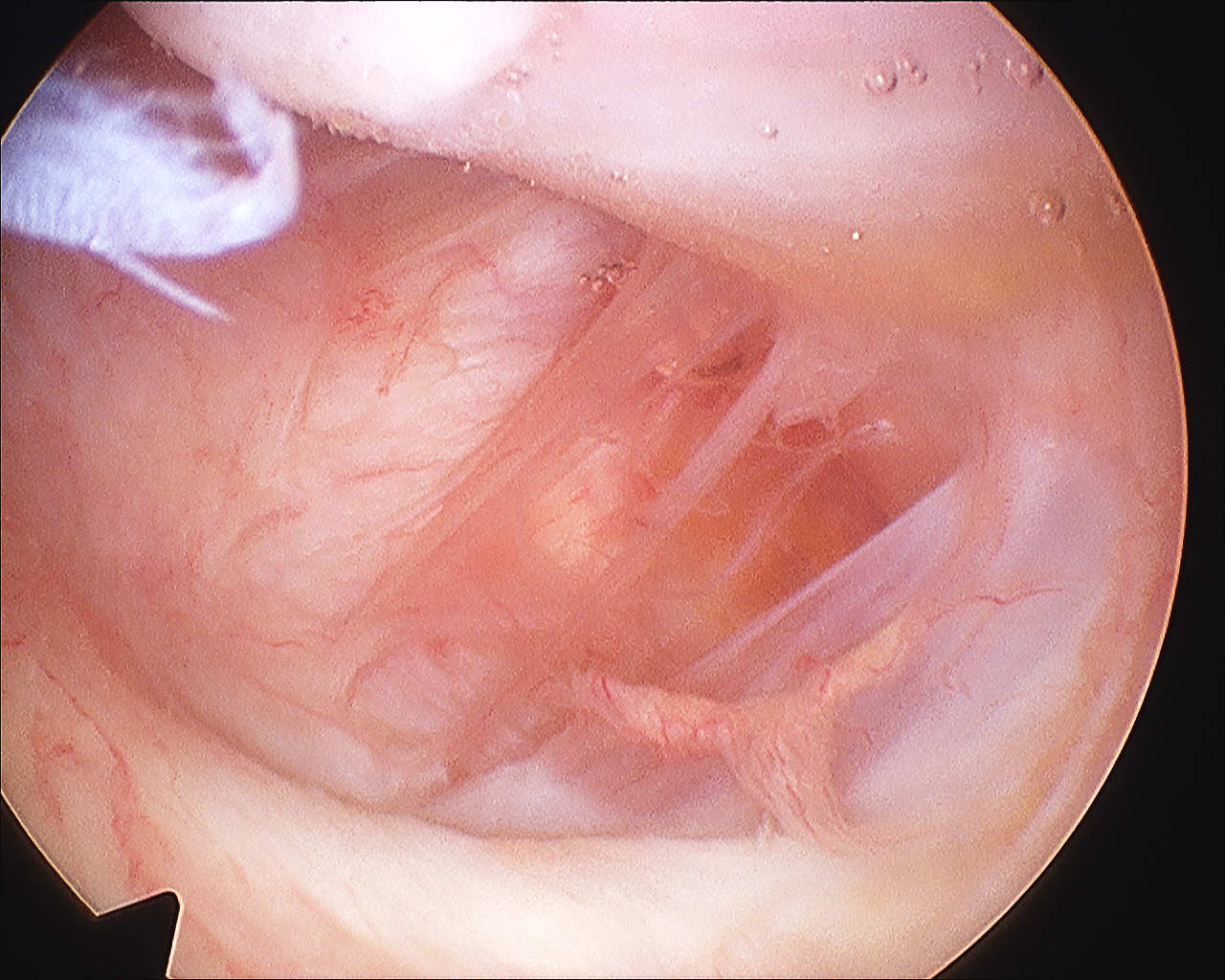
Humeral Avulsion of Glenohumeral Ligament
Incidence
Bokor et al JBJS Br 1999
- 514 cases surgical treatment traumatic instability
- incidence 7.5%
- 25% associated SSC tear
- likelihood of HAGL if no Bankart or MDI 27%
Latarjet / Bristow
Bristow
Concept
Non-anatomical bony block
- transfer of coracoid process through subscapularis
- dynamic anteroinferior musculotendinous sling
- provides subscapularis tenodesis
- preventing lower portion from displacing proximally as arm abducted
- when shoulder in vulnerable position abduction and ER