
Definition
Infantile tibia vara
- progressive varus deformity of knees
- secondary to abnormality of medial upper tibial physis
Epidemiology
African descent / males / obesity
Etiology
Disruption of normal medial endochondral bone formation
Unknown
- no consistent inheritance pattern
- ? due to abnormal compression on medial side of proximal tibial physis
Types
| Infantile | Adolescent |
|---|---|
|
Onset 1 - 3 years Bilateral Most common |
Onset > 6 years Unilateral Rare |
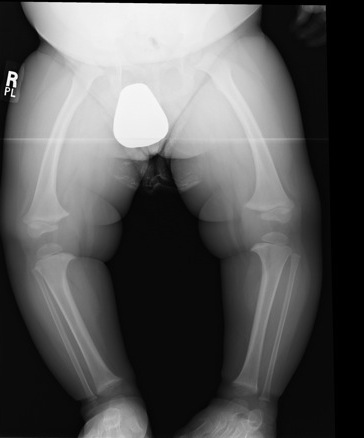
Clinical
Bilateral & symmetrical bowing
- age 1 - 3
- walking
- normal physiological varus should resolve by age 2
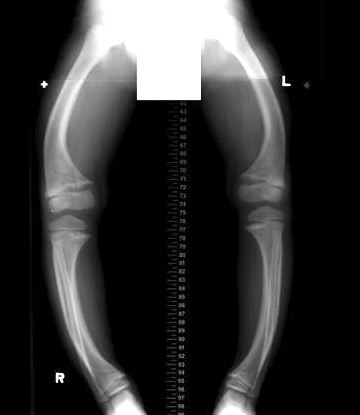
Varus knee
Tibial torsion
X-ray

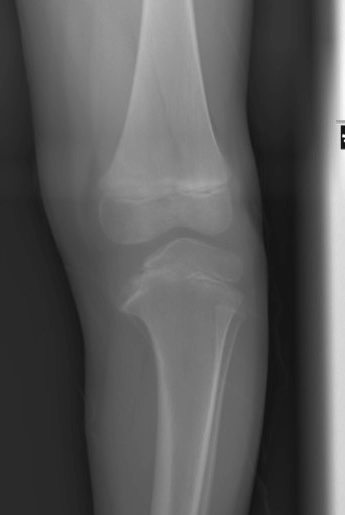
Findings
- medial beaking of the epiphysis
- widened and irregular medial physis
- medial slope of the epiphysis
- metaphyseal varus



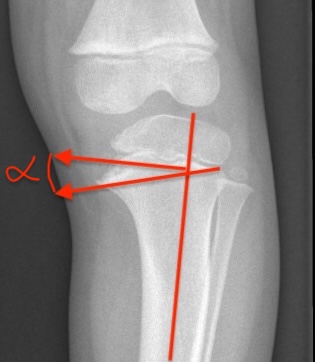
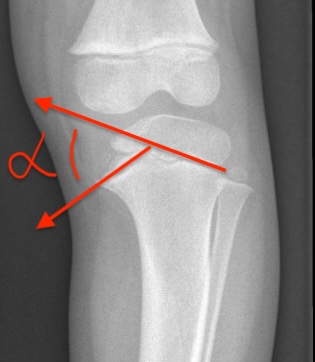
| Metaphyseal-Diaphyseal Angle | Medial physeal slope |
|---|---|
|
Line perpendicular to axis of tibia Line through medial and lateral metaphyseal beaks
|
Line through medial physis Line through lateral physis |
|
Physiologic bow legs < 11° Blount's > 11° Definitive Blount's > 16o |
High risk of progression if > 60° |
 |
 |
CT
Used to identify presence of physeal bar
Langenskiold Classification
Six stages
- stages I - III: reversible with bracing
- stages IV - VI: permanent damage to eiphysis / need surgery
| Stage I | Stage II | Stage III |
|---|---|---|
| Medial beak | Medial saucer shaped defect | Develop step |
| Age 2 - 3 | Age 2 - 4 | Age 4 - 6 |



| Stage IV | Stage V | Stage VI |
|---|---|---|
|
Narrow physis Step deepens |
Medial epiphysis splits into two Physeal bar |
Medial growth arrest Develop severe varus |
| Age 5 - 10 | Age 9 - 11 | Age 10 - 13 |


Differential diagnosis

Rickets Achondroplasia
Physiological varus - normal growth plate, metaphyseal-diaphyseal angle < 11°
Ricket's - widened physes / cupped metaphyses / flared distal distal
Metaphyseal chondrodysplasia
Achondroplasia
Trauma / tumour / infection
Osteogenesis imperfecta
Juvenile rheumatoid arthritis
Natural history
Progresses to severe osteoarthritis by early adulthood
Disease progression
- metaphyseal-diaphyseal angle >16° - 95% chance of progression
- metaphyseal-diaphyseal angle < 11° - 95% chance of spontaneous resolution
- metaphyseal-diaphyseal angle < 11 - 16° - close observation
Management
Algorithm
Depends on
- age of child
- stage of disease
1. <2 years
Observe
2. 2 - 3 years & Medial Physeal Angle < 60°
KAFO Single Medial upright
- free ankle with no knee hinge
- flexion limited
- knee cuff pulls it into valgus
Full-time bracing successful > 50%
3. Age > 3 years / Progression in Brace / Medial Physeal Angle > 60°
Aim
- correct varus and internal rotation deformity
Options
A. Lagenskiold I - IV
- osteotomy
- guide growith
B. Lagneskiold V / VI
- take down bar and osteotomy or
- epiphysiolysis + medial metaphseal osteotomy
Langenskiold Stages I-IV Surgical Management
1. Osteotomy
Aim
- restore alignment
- deformity reversible
- if restore physiological valgus (7o) then resolution is usual for I & II / possible for III & IV
Type of osteotomy
A. Opening / closing wedge
B. "Smiley" upside down dome
C. Oblique osteotomy
- Rab biplanar oblique osteotomy
- fix with single screw
Osteotomy Technique
Performed distal to TT
- closing wedge simplest but upside down dome has least shortening
- must osteotomise fibula
- usually want to correct IR deformity at same time
- must release anterior compartment to prevent compartment syndrome
- desired valgus & ER achieved
- fixation with K wires or screw
- POP post operatively
Recurrence after osteotomy
1. Obese
2. > Stage III
3. Medial physeal slope > 60°
4. Age
- > 5 y = 76%
- < 5 y = 31%
2. Guided growth / 8 plate
Now common mechanism of treating condition
3. Osteotomy and external fixation
Langenskiold Stages V & VI
Issue
Irreversible
- need to address physis as well as osteotomy
- usually total physiodesis
- overcorrection 10°
Surgery
- must do fibula osteotomy as well
- usually perform total physeodesis of ipsilateral side
- always perform fasciotomy
- may need to realign epiphysis in severe forms with large medial-physeal slope
- consider epiphysiodesis of other side to address LLD
Options
1. Medial Metaphyseal Elevation Osteotomy
Indications
- Grade V

2. Physeal Bridge Resection (physeolysis) + Osteotomy
Indications
- Grade VI
- bridge < 30% of physis
Technique
- excise bar where CT shows a bridge
- Insert fat into defect
3. Lateral Hemi-epiphysiodesis + osteotomy
Indications
- grade VI
- bridge > 30%
Technique
All need fibula osteotomy
All need prophylactic compartment release
Complications
Compartment syndrome - must prophylactic release
Recurrence of varus - usually secondary to physeal bar
LLD
OA
Adolescent Type
Management
Wait till skeletal maturity, then HTO