Acute management
EMST / ATLS Principles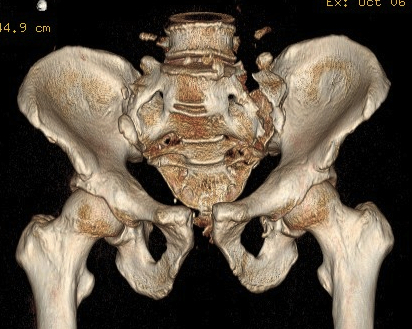
Usually polytrauma
- 10% mortality
Aims
1. Volume replacement
2. Reduce pelvic ring
3. Stop exsanguination
- external stabilisation / surgery / embolisation
Associated Local Injuries
Arterial bleeders
Usually polytrauma
- 10% mortality
Aims
1. Volume replacement
2. Reduce pelvic ring
3. Stop exsanguination
- external stabilisation / surgery / embolisation
Arterial bleeders
Unusual anatomic convergence of ilium, pubis and ischium
- covered entirely by hyaline cartilage
- except at acetabular fossa, which is the site of attachment of the ligamentum teres
- deepened by peripheral fibrocartilage labrum
2 column theory (Letournel and Judet)
Anterior Column
- superior pubic ramus
- anterior acetabular wall, anterior dome
Non Operative
- < 2.5 cm displacement
- indicates SS and ST intact
- nil posterior opening
Operative
1. > 2.5 cm
- single anterior plate through Pfannelstiel incision
2. Posterior SIJ disruption
- reduction and posterior stabilisation
- usually with SI screws
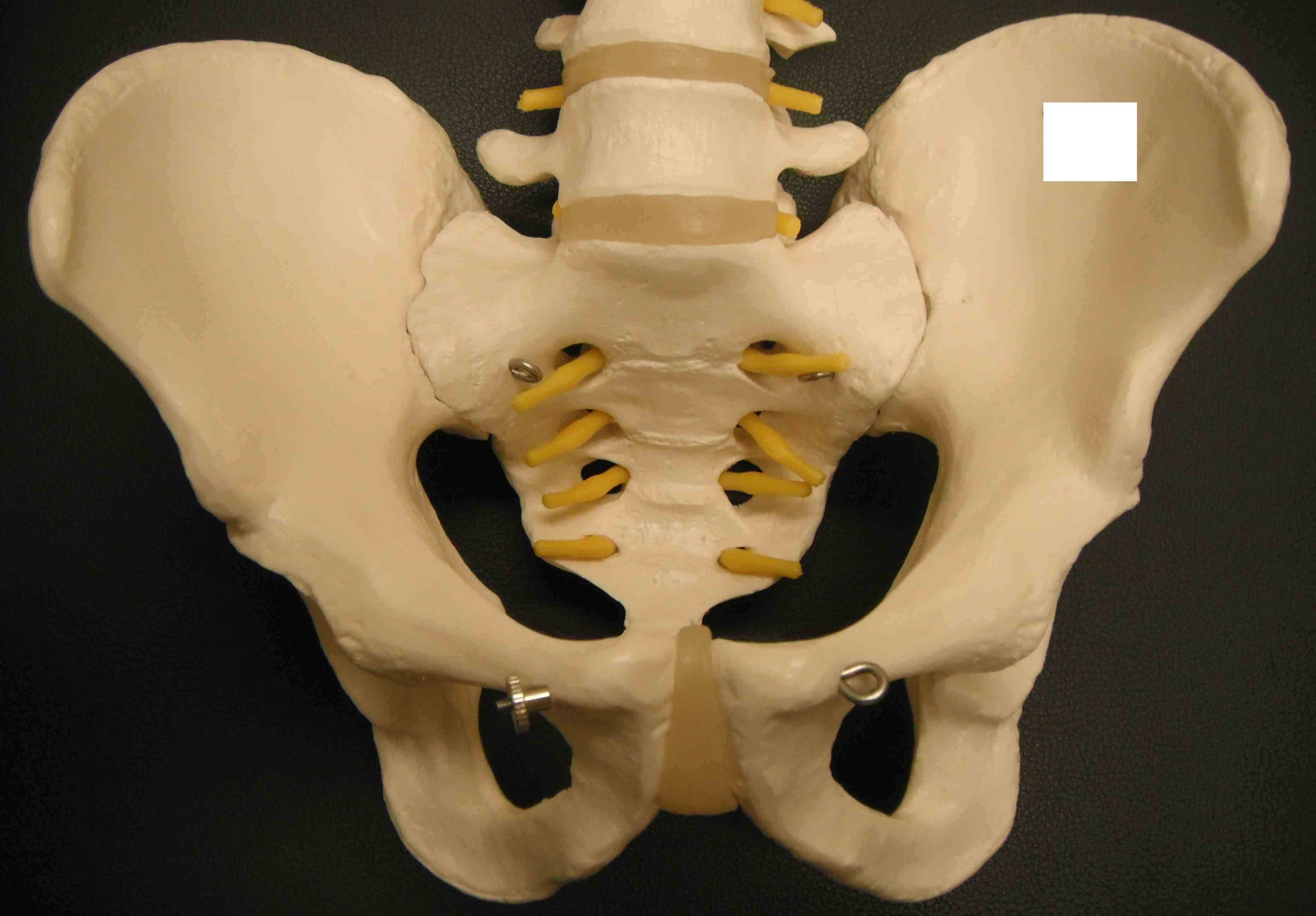
Pelvis is a true ring
- any anterior fracture must have a posterior injury as well
- integrity of the posterior sacroiliac complex is key
2 innominate bones + sacrum
Symphysis pubis < 5mm
SI joint 2-4 mm